
The statue in front of Lusaka Eye Hospital of Jesus healing a blind man was donated by a branch of the Lions Bank in Germany and Christian Blind Mission



I've gotten fairly accustomed to the schedule and routine here at the eye hospital, which basically breaks down like this:
Monday- Switch between clinic with Dr. Celestine, a Rwandan ophthalmologist, and surgeries with Dr. Yoo
Tuesday- Surgeries with Dr. Celestine and Argent, an ophthalmic surgeon (equivalent in training to a PA who has had training in ophthalmologic surgeries)
Wednesday- Clinic with Dr. Celestine
Thursday- Clinic with Dr. Yoo
Friday- Clinic with whoever
Every morning we'll start off with a devotional with the rest of the hospital staff. We'll sing some hymns, sometimes hear a mini-sermon, then practice some worship a cappella. One of the songs we're learning, unofficially titled "Basumina," was composed and arranged by one of the hospital staff, an outgoing, exuberant guy named Jones.

Jones- one day he told me to call him by another name but I forgot the other name

The staff of Lusaka Eye Hospital in front of the hospital bus
On Thursdays, we have informational talks, such as the one pictured below by a member of the hospital staff on Zika virus.

There's at least twenty staff members that ensure Lusaka Eye Hospital runs smoothly. Linda is the Human Resources manager who coordinates almost everything at the hospital- including travel arrangements for international visitors such as myself! Mrs. Sharpeza is the cleaning lady for the hospital and is always going around the hospital with a smile and upbeat spirit.

Linda hard at work

Mrs. Sharpeza who keeps the hospital clean
Apparently the hospital was rife with problems before Dr. Yoo came in- the hospital was deeply in debt, thanks in part to an embezzling employee, and inefficiency was the name of the game. Once Dr. Yoo took over as an ophthalmologist and the administrator of the hospital, Lusaka Eye Hospital has gained in reputation not only in Zambia but in Loma Linda as well as a success story of healthcare in the developing world. The hospital is now no longer in debt, and is fully self-sufficient. This is due in part to a switch to a business model similar to that used by Aravind Eye Care in India, where the profit made from paying patients covers the costs of services for those patients who cannot afford to pay. Outside organizations do fund certain programs, such as Loma Linda's "See It Forward" program in which patients having cataract surgery at Loma Linda can elect to fund cataract surgery for patients without the means to do so at Lusaka.

Some patients being sponsored by the See It Forward program waiting outside the operating theater for their cataract surgeries
The patients at Lusaka Eye Hospital present with a number of different ophthalmologic conditions, but the majority of the patients I've seen have come in for refractive error (aka they need glasses), cataracts, glaucoma, and diabetic retinopathy (unfortunately- Dr. Yoo says diabetes is on the rise here). In Dr. Yoo's clinic, the majority of the patients I've seen have corneal issues like corneal ulcers (Dr. Yoo got some excellent corneal training, after all!) and pediatric cases like cross-eyes (called zambiopia... err, amblyopia).
The patients here run the whole socioeconomic spectrum. One day in clinic, a man came in who had essentially lost vision in both eyes- one due to trauma, the other due to an infection called chorioretinitis. Dr. Celestine explained to me how this man had basically squandered all his money, his relatives had disowned him, and Dr. Celestine now paid for the man's medications. Then the next patient who came in was the ambassador from Burundi to Zambia!

(Left to right) The Burundian ambassador to Zambia, the ambassador's security guard/body double/friend (??), and me
One morning an 18 year old girl studying at a nearby university came in with her father, complaining of visual loss in her right eye for two days. She told me she was studying medicine and that it would take her seven years to finish, as the undergraduate years and medical school years are combined here in Zambia. After taking a look at her eye with the slit lamp, Dr. Celestine urged me to take a look as well. "She has CMV retinitis," he informed me while also noting her skin findings which seemed to be those caused by herpes zoster ophthalmicus. Sure enough, the characteristic white lesions and hemorrhages were in plain view when looking at the back of her eye through the slit lamp.

CMV retinitis when viewed with a slit lamp and lens
Something seemed a bit off to me. "Does this mean she's immunocompromised?" I asked Dr. Celestine when the patient had left the room, struggling to understand how this young, seemingly healthy girl could have a cytomegalovirus infection of the eye, which typically affects people with advanced HIV. Dr. Celestine spoke with the girl's father in private and discovered that the girl did, in fact, have HIV which had only been diagnosed a few days ago. To further add to the tragedy, Dr. Celestine felt that the disease was too advanced for treatment, so he did not prescribe the girl the typical medication for CMV retinitis as he believed her vision was likely lost forever.
-----
I saw one case of a condition called central serous chorioretinopathy- it's thought to be triggered by stress and is a rare condition typically only found in males 20-50 years old.
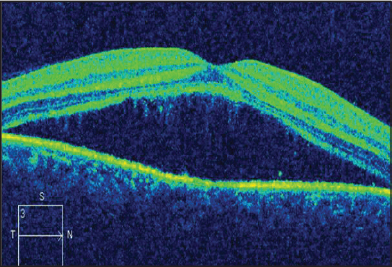
CT scan of the back of a patient's eye showing central serous chorioretinopathy
-----
I've also seen a few young patients with retinoblastoma who come in and require enucleation (removal of the eye). It's an incredibly difficult decision for parents to decide to make the potentially life-saving decision to have their child's eye removed. It saddens me that these children don't have access to treatment modalities such as chemotherapy which are employed at eye cancer treatment centers in the US, while simultaneously optimistic for a future in which these treatments will be available for children like those in Lusaka.

one common sign of retinoblastoma in a child is a white pupil
Still, it makes me hopeful that at least these retinoblastomas are being caught before they end these children's lives, as recent estimates peg the survival rates for children with these tumors at roughly 35% in Africa.
-----
Surgeries take place in the "theater" here, where Dr. Yoo, Dr. Celestine, and Argent do everything from small incision cataract surgery to corneal transplants to pterygium excisions. I had actually expected to see more patients with trachoma, but I've only seen one surgery for trichiasis here, which is a condition caused by trachoma in which the eyelashes grow inward and potentially scar the cornea. Argent explained that trachoma is found mostly in the more remote areas of Zambia, and patients usually don't come for treatment until their conditions have reached an advanced stage.


Patients awaiting cataract surgery

Ophtho resident An learning how to do manual small incision cataract surgery under the guidance of Dr. Celestine and Argent
Our lunch is provided daily by the hospital and is typically comprised of rice, nshima (one of the national foods of Zambia made of maize- think the cornmeal part of a tamale but starchier and less flavorful), vegetables (including sweet potato leaves on some days), and some sort of protein (i.e. eggs or veggie-meat).

A typical lunch
I noticed my Zambian coworkers eating the nshima by smashing it up into a ball in their hands, then picking up some food against it before putting the mini-meal in their mouths. I asked them to show me how to do it without realizing that there's actually an art to smashing nshima, using your four fingers as a single unit to press it into the palm of your hand, while keeping your palm and thumb stationary. My coworkers definitely had a good laugh when I tried it the first time, my fingers and nshima flying everywhere as I smashed away.

NOT the right way to smash nshima

Tasted kind of like a smashed-rice ball


































